
A Providence St. Joseph Health subsidiary is trying to close a population representation gap in important medical research.

Black, Latino and American Indian people are underrepresented in colorectal cancer studies, largely because they are poorly represented in the bio-repositories — or repositories of biospecimens — used in that research. These marginalized, ethnically and racially diverse populations also are less likely than white people to be screened for colorectal cancer, and they have worse outcomes from the condition. There are similar disparities for many other medical conditions. All this is according to researchers with Providence's Health Research Accelerator.
Those researchers are trying to better understand and address these disparities.
"If we limit our research to white people, what are we missing?" asks Kristi Roybal, a clinical research scientist with the accelerator and lead author of a study that ran in the Journal of Community Genetics in January. She notes that "there may be meaningful differences" among different populations in how colorectal cancer and other conditions originate, how they develop and evolve, how they impact people and how prevention and treatment are approached.
Roybal says when it comes to these disparities, "We are striving to do better. So: How can we be more culturally responsive? We need to understand who our patients are ... We are trying to understand how to meet them where they are."

"Our work is actionable," adds Staci Wendt, director of research for the Health Research Accelerator, which Providence founded in 2021 to harness the vast amount of information contained in the health system's cloud-based data warehouse. The focus of the accelerator's research is reducing disparities and accelerating innovations to improve patient care and outcomes. The accelerator has about 30 dedicated staff.
Skewed data
In the study Roybal led, she and her fellow authors say analyses have found that "racial and ethnic inequities in diagnosis and mortality ... persist, as marginalized racial and ethnic groups have more risk factors, are less likely to receive screening and are more likely to be diagnosed with late-stage" colorectal cancer. Roybal and team cite research that found Black Americans have the highest incidence and mortality for colorectal cancer, compared with all other racial and ethnic groups.
Roybal and her co-authors also cite research that found that nearly 90% of individuals in large-scale genomic studies and biorepositories — which contain biospecimens such as tissue, blood, plasma and urine — are of European ancestry.
Dream team
The accelerator began its work around colorectal cancer disparities using a grant from the nonprofit fundraising organization Stand Up To Cancer. The goal was to improve screening rates among marginalized people.
The researchers assembled what they called "the colorectal cancer health equity dream team," which included experts in three communities — Greater Boston, Los Angeles and tribal nations in South Dakota — to determine how best to connect with community members and encourage them to get screened. The researchers conducted the outreach in areas with racially and ethnically marginalized populations.
As part of their role on the dream team, the accelerator staff deployed community health action teams made up of specially trained community members to undertake a campaign tailored to local residents in Los Angeles. They conducted longitudinal research on what works best.
Trust gap
The accelerator researchers secured a second Stand Up To Cancer grant to collaborate with the University of California Los Angeles and Massachusetts General Hospital to conduct the Roybal-led qualitative study between 2022 and 2024. The study's purpose was to identify information needs and culturally appropriate approaches to biorepository recruitment, Roybal says.
The researchers first interviewed experts from several states who had experience recruiting diverse participants into biospecimen research. They then assembled 21 focus groups in the same communities where the dream team focused its work. One hundred and one Black, Latino and American Indian people participated in the focus groups.
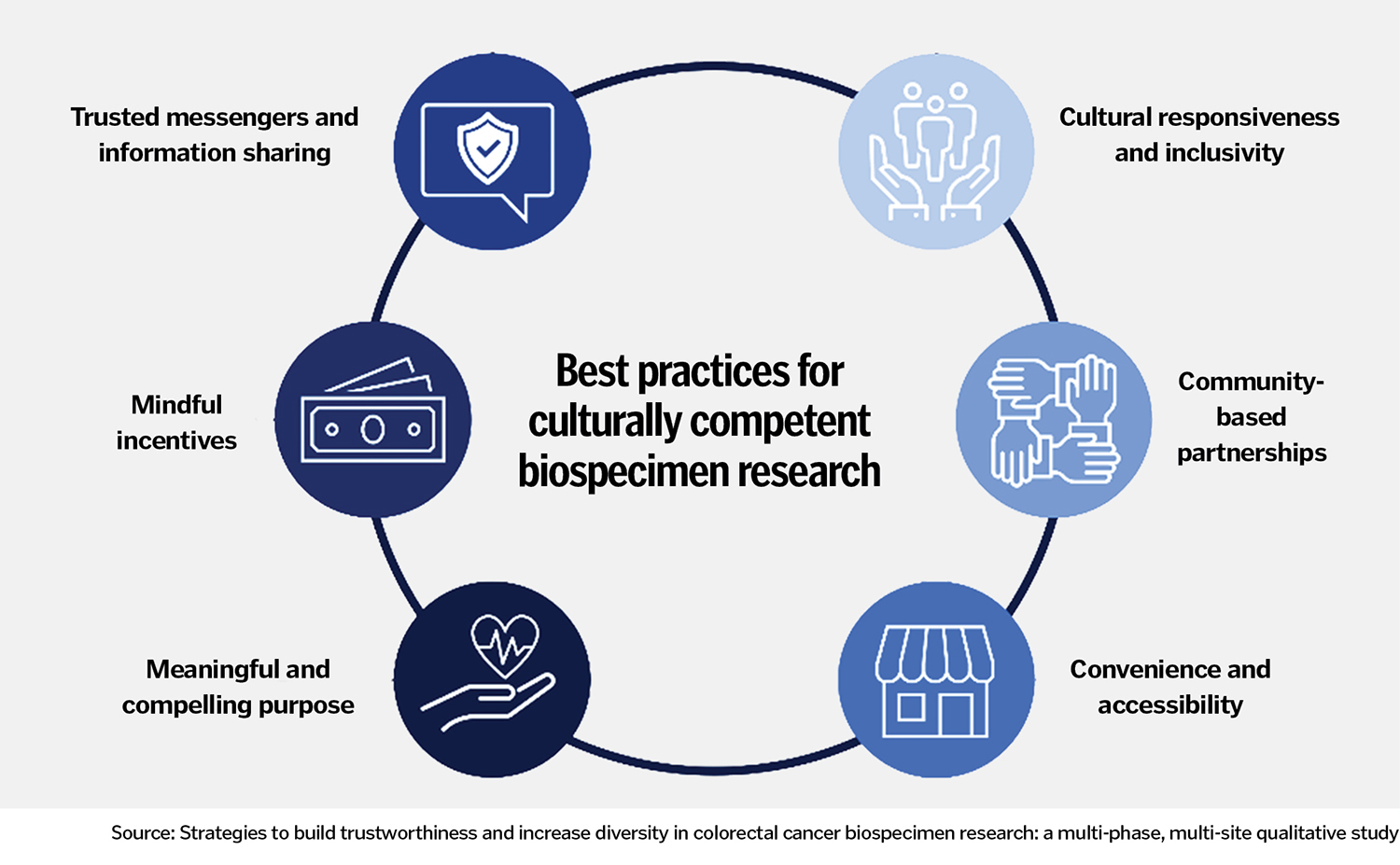
The study identified six themes that illuminate how researchers can address the "trust gap" that underlies the low representation of these communities in biospecimen research:
- Cultural responsiveness and inclusivity: Diversity and inclusion should be central to any research project, study respondents said.
- Community-based partnerships: Organizations that are well integrated in and respected by the community can be a pathway to connecting with community members.
- Convenience and accessibility: Researchers should make it easy and cost-free for people to take part in their studies.
- Meaningful and compelling purpose: Researchers should be explicit about how participation in the research will benefit the local community.
- Mindful incentives: If incentives like gift cards are provided, they should be usable and valuable to the participants. For instance, a grocery gift card is not valuable if individuals can't get to a store easily.
- Trusted messengers and information sharing: In communicating about the research, the researchers should engage trusted medical providers and community members to deliver the information in an authentic way.
Practical uses
The accelerator team has used their findings to produce a tool kit, "Best Practices Framework for Culturally Competent Biospecimen Research." It puts learnings about the trust gap study into easily understandable terms and provides prompts and suggestions to guide researchers and others in ensuring diversity in biomedical research.
Roybal and Wendt say they are optimistic that this work will help increase the representation of Black, Latino and American Indian communities in biospecimen research.
Roybal says doing so is critically important because a nuanced and comprehensive understanding of the biology of people's diseases is needed, especially for advancing precision medicine treatments. If study participants' biospecimens and medical information are not representative of the population generally, researchers will have an incomplete picture and understanding of the disease under study and of how to prevent, detect and treat it in the future.
Roybal and Wendt also hope the research the accelerator is conducting will prompt scientists and others to think about some of the tensions at play in medical research, particularly involving racially and ethnically marginalized communities. For instance, are researchers considering: How have harmful medical research practices impacted perceptions of the trustworthiness of researchers among Black, Latino and American Indian communities? Are the funders of medical research — including drugmakers — trusted by potential research participants? Are they trustworthy? Will racially and ethnically marginalized people reap the benefits of the biospecimen research studies they participate in?
Such questions may spur future accelerator research.
"Often, we frame trust or mistrust as an individual issue instead of an issue about health systems taking responsibility for how we shape how people perceive us," Roybal notes. "It's a call for demonstrating our trustworthiness. It's on us as researchers to demonstrate we can be trusted."